202406241357
Status:
Tags: ECG
Ventricular tachycardia
- Rate >120bpm
- precordial concordance V1-6
- AV Dissociation
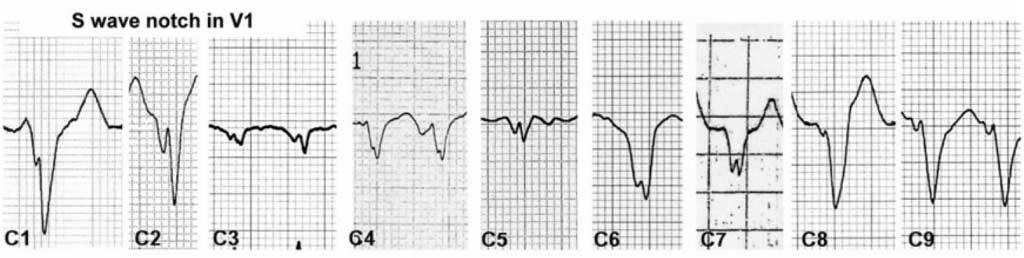
- Josephson's sign V1-2
- V1: FAT initial R wave
-
40ms
- could be rabbit ear
-
- aVR: FAT wave to begin with
- Lead II : R wave peak time >=50ms
- FAT R wave
VT Score
uses 7 criteria
A specificity of 100% is reached when >=4 criteria are satisfied.
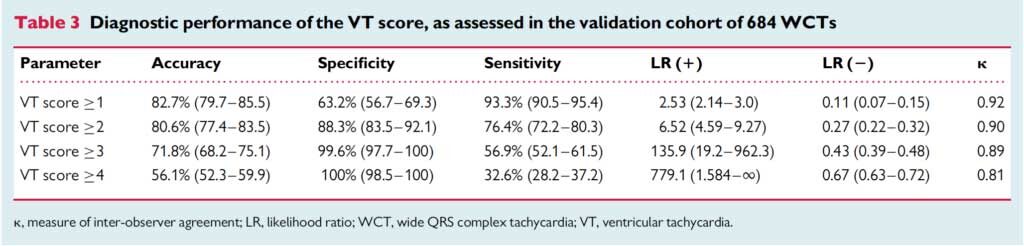
- V1: Dominant initial R wave
- V1 or V2: initial r > 40ms
- V1: notched S = Josephson's sign
- aVR: initial R wave
- lead II: R wave peak time >=50ms
- V1-6 concordance
- AV Dissociation
Josephson sign
V1 notched S
4 main types of VT
Non-sustained Monomorphic VT
- Rate > 120-130 bpm
- Lasts <30s, no associated hemodynamic instability
- Key to treatment is to look for and treat the underlying cause
- Cardiac ischemic, hypoxia, electrolyte abnormalities, PE, etc.
- Cardiac ischemia may induce sustained or non-sustained monomorphic VT in the presence of a myocardial scar
- Empiric antiarrhythmic therapies are probably not indicated. No antiarrhythmic drug is suitable for primary prevention of cardiac death except for beta blockers
Sustained Monomorphic VT
- Rate > 120-130 bpm
- Lasts at least 30 seconds or produces hemodynamic instability
- Usually associated with scar from prior MI or other anatomic pathology
- Can sometimes be associated with ACS
- Treatment with antiarrhythmics medications or cardioversion
- Sedation and cardioversion are the preferred treatment
- Medications: procainamide >> amiodarone
- Treat the underlying cause
Generic polymorphic VT (normal QTc – PVT)
- Normal QTc vs. Torsades which is associated with prolonged QTc
- Causes
- Usually associated with cardiac ischemic/ACS, also seen with Brugada syndrome and other miscellaneous reasons
- In the absence of a Brugada pattern or other clear cause, consider and treat for cardiac ischemia until proven otherwise.
- Treatment
- When persistent, patients are usually unstable. Proceed with sedation and defibrillation, then…
- Treat for ACS and seek urgent revascularization when possible if an occlusion MI is thought to be the cause
- Beta blockers after conversion are helpful if episodic bradycardia or heart block is not an issue
- In cases of concurrent bradycardia or complete heart block, avoid beta blockers (including amiodarone which has beta blocking properties), lidocaine may be the best option in some cases (easy to dose, works quickly, does not cause hemodynamic instability)
- When persistent, patients are usually unstable. Proceed with sedation and defibrillation, then…
Torsades de pointes (type of PVT a/w long QTc)
- At significant risk when QTc ≥ 500 ms in sinus rhythm
- Note: Diagnosis is NOT based on morphology alone. All forms of PVT may have a “twisting of the points” appearance in some leads. Scrutinize the QT interval before and after rhythm conversion.
- Causes
- Electrolytes: Hypomagnesemia, Hypokalemia, Hypocalcemia
- Hypothermia
- Medication and drug induced
- Elevated intracranial pressure
- Congenital long QT syndromes
- Treatment
- Most episodes of torsades are self-limited. If persistent, defibrillate when unstable and give magnesium bolus if defibrillation is unsuccessful or to prevent recurrence
- When in doubt between generic PVT vs. torsades, defibrillation and empiric Mg2+ are reasonable options
- When intermittent, give Mg2+ slow IV push and infusion even when serum magnesium levels are normal (monitor for hypermagnesemia and toxicity during infusion)
- Overdrive pacing (shortens the QTc) may be necessary
- Electrically pace at 100-120 bpm
- Chemically with isoproterenol, dopamine, or epinephrine
- Avoid procainamide and amiodarone (will further prolong QTc)
- Avoid beta blockers in acquired forms (will further prolong QTc)
- Discontinue any QT prolonging medications and raise serum potassium levels to high-normal range, while looking for underlying causes
- Most episodes of torsades are self-limited. If persistent, defibrillate when unstable and give magnesium bolus if defibrillation is unsuccessful or to prevent recurrence
Mimics:
metabolic (hyperkalaemia) / tox (Na channel blocker):
- Suspect when…
- HR is too slow (< 130 bpm) or
- QRS is too wide (> 200 ms)
VT in cardiac arrest
Amiodarone
- 300mg IV bolus
- 150mg prn
- ROSC → 1mg/min infusion
Procainamide - probably not useful in cardiac arrest
- long time to establish loading dose
ß blockers - propranolol
- non-selective
- 1-3mg IV Q5min
- Max 5mg
- esmolol
- ß1 selective
- 500µg/kg IV bolus
- 50-300µg/kg infusion
- (metoprolol)
- probably not as effective
- 5mg IV Q5min
- Max 15mg
Lignocaine
- 1-1.5mg/kg bolus
- 2nd dose: 0.5-1mg/kg
- ROSC → 1-4mg/min infusion
- may be first line in 2 scenarios:
- acute cardiac ischaemia
- TdP
- ∵ shorten QT interval
Mg
- ∵ shorten QT interval
- 2g IV MgSO4 upfront
- TdP → 4g IV bolus followed by infusion
- target Mg 2.2-2.5mg/dL