As a Nephrologist, Why D...
Highlights
- As a Nephrologist, why do I love vasopressin? Particularly when I see patients in the CCU?
My ode to vasopressin in a 🧵
#medtwitter #cardstwitter #nephtwitter @MedTweetorials (View Tweet)
- Right off the bat let's acknowledge that the following trials show no mortality benefit in critically ill patients with vasopressin. But that's not the point - we only care about the kidneys right now because I'm a Nephrologist. (View Tweet)
- Before we get to hearts we need to borrow from the sepsis literature.
First a small study from 2002
💥24 pts w/septic shock
💥vasopressin v norepinephrine x4 hrs, titrated to BP
💥Vasopressin group = better UOP and CrCl
https://t.co/iYoRq9Q80h

 (View Tweet)
(View Tweet)
- Lauzier et al from 2006
💥23 pts w/septic shock
💥Vasopressin v NE. Equal BPs at 48 hrs, however NE required in 36% of vaso patients to do so
💥Better CrCl in the vasopressin group
https://t.co/ThCDmOOUg0
 (View Tweet)
(View Tweet)
- Morelli et al 2009
💥45 pts w/septic shock
💥terlipressin v vasopressin v norepinephrine
💥Again worse kidney function, by creatinine criteria, in the norepinephrine group
https://t.co/R4AeShXLay
 (View Tweet)
(View Tweet)
- In 2008 in the NEJM we got the VASST trial. 778 pts w/septic shock randomized to vasopressin or NE. No difference in mortality.
BUT: Gordon et al performed a post-hoc analysis and found that "at risk pts" (creatinine x1.5) had lower rates of progression of AKI with vasopressin
 (View Tweet)
(View Tweet)
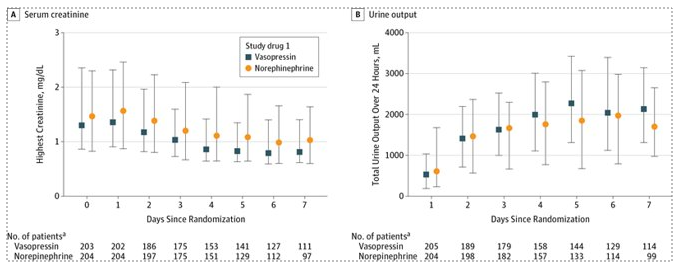
- Same group published the VANISH trial in JAMA in 2016.
💥409 pts w/septic shock
💥vasopressin v NE (2x2 design with steroid arms as well)
💥NO difference in kidney-failure free days between groups
🔥BUT better UOP and decreased use KRT in the vaso group
https://t.co/70e8CkAmlg
 (View Tweet)
(View Tweet)
- How about vaso post Cardiac Surgery? Enter the VANCS trial from 2017.
💥330 pts with vasoplegic shock (MAP<65 and CI>2.2 resistant to fluids)
💥vaso vs NE
💥Again, better kidney function in the vaso group
https://t.co/wIzBhDgpJW
 (View Tweet)
(View Tweet)
- OK, so there's seems to be evidence to suggest that vasopressin improves kidney outcomes. But how do we extrapolate to the CCU?
💡In low flow states, RBF falls well before GFR due to the kidney's ability to autoregulate
🔥Primary mechanism for this is efferent vasoconstriction
 (View Tweet)
(View Tweet)
- Borrowing from HRS. Relationship b/w RBF and BP is altered during SNS activation (which happens with CRS as well) - with a rightward shift in the renal autoregulatory curve so RBC is critically dependent on BP.
🔥Concept here is RPP (MAP-CVP) and should be considered in all pts (View Tweet)
- 💥While NE constricts both efferent/afferent arterioles - vasopressin appears to exert a preferential effect on the efferent arteriole, which may explain the beneficial kidney outcomes
We use this to our advantage in certain cases of diuretic resistance
https://t.co/3Jkra9gq5m

 (View Tweet)
(View Tweet)
- This may be particularly useful in pts with right heart failure since you're not as concerned about afterload with a presumably functioning LV.
💥Vaso does not appear to impact the pulm artery, whereas NE exerts a vasoconstrictive effect
https://t.co/q8Hir6R0AG
 (View Tweet)
(View Tweet)
- Conclusions:
💥Vasopressin assoc with better kidney outcomes in critically ill pts
💥Preferential efferent vasoconstriction may explain the above. Can use this in certain cases of DR
💥RPP (MAP-CVP) should be considered in all pts
💥May be particularly useful in RV failure
END. (View Tweet)