1/ *Can We See Torsades...

Highlights
- 1/ Can we see Torsades coming?
A few months ago, I had the chance to study the rhythm changes leading up to an episode of Torsades. Discussed here -
https://t.co/nddhsIAcD4
This helped me pick up some "warning signs" that may help facilitate early recognition.
#tweetorial (View Tweet)
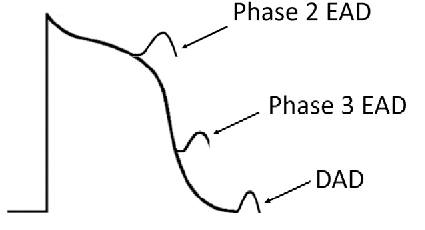
- 2/There are 3 critical substrates for Torsades:
(i) Prolonged action potential (long QT)
(ii) Early afterdepolarizations (EAD)
(iii) Dispersion of repolarization (DR)
(i)A long QT is essential but not sufficient. E.g. Amiodarone prolongs QT but reduces DR - low risk of Torsades. (View Tweet)
- 3/ (ii) EAD = depolorization during phase 2/3. In long QT, a longer phase 2 period increases the chances of EADs. However, not every long QT develops EAD so other mechanisms may be involved.
(iii) DR = heterogenous repolarization properties within the myocardium: PMID: 16253930.
 (View Tweet)
(View Tweet)
- 4/ Although torsades is "initiated" by EADs, it is likely "maintained" by reentry mechanisms facilitated by DR.
Now let's focus on EADs. They are responsible for the "R" in the "R-on-T". They are also likely responsible for some of the EKG changes leading up to Torsades. (View Tweet)
- 5/ Again, EADs don't always result in Torsades (if not followed by reentry). Importantly, their electrical effects can be picked up on a surface EKG. The pattern of EKG findings depend on whether the EAD was propagated (technical term = triggered activity) or not. (View Tweet)
- 6/ (i) EAD not propagated - this would result in repolarization abnormalities - the giant T-U wave (T and U waves are often fused and difficult to distinguish).
This has been systematically studied: PMID: 19573731. Abnormal T-U waves directly preceded Torsades in 34/35 patients!
 (View Tweet)
(View Tweet)
- 7/(ii) If the EAD is propagated -this would result in a PVC right after the giant T-U wave
PVCs are usually accompanied by ST-T aberrancies (just like bundle branch blocks). However, you combine this with EADs and it results in "bizarre" ST-T changes.
Example from that article
 (View Tweet)
(View Tweet)
- 8/ Importantly, since EAD is facilitated by longer action potential duration (APD), the amplitude of the 'post-pause' EADs would be higher.
This can happen when a PAC/PVC resets the sinus node and the next sinus beat is delayed. This delayed beat will have a longer APD.
 (View Tweet)
(View Tweet)
- 9/ If the amplitude of the post-pause EAD is high enough, it may propagate and cause a PVC. This PVC will reset the sinus node and cause another pause and so on.
This produces a bigeminal pattern called "short-long sequence", the initiation of which was demonstrated in our case.

 (View Tweet)
(View Tweet)
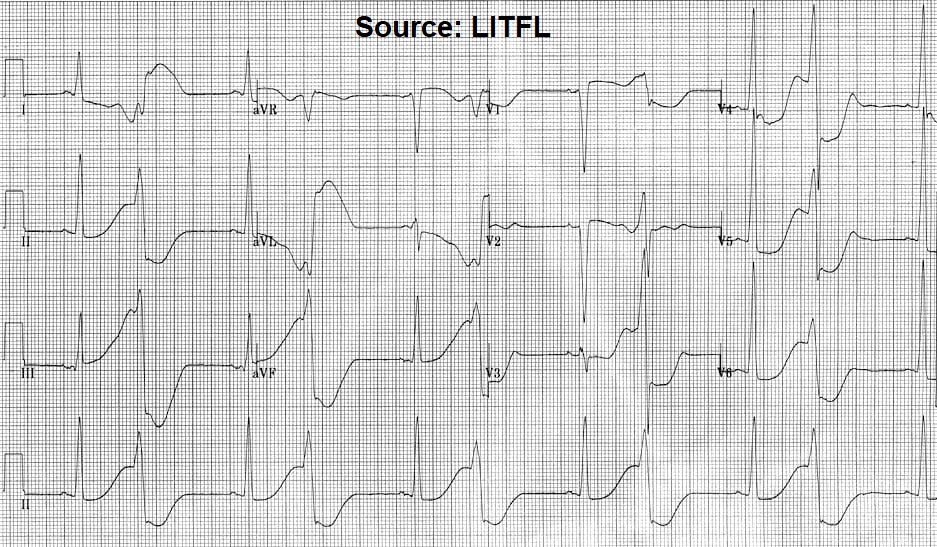
- 10/ When you see this pattern, Torsades is absolutely imminent.
Found a similar example on LITFL - https://t.co/ttnhCq0lbX
A few weeks later I had saw this pattern again in a patient who was started on scheduled Reglan. 2 g Mag over 10 minutes resulted in obvious improvement.
 (View Tweet)
(View Tweet)
- 11/ I have no doubt in my mind that patient would have had Torsades had I not administered the Mag.
Side-note -
It's also important to not confuse this pattern with ischemia. Although the PVCs may have discordant ST changes, careful assessment of the sinus beats will be helpful. (View Tweet)
- 12/ Summary:
(i) As telemetry is ubiquitous in the ICU, an astute pair of eyes may be able to 'see Torsades coming'
(ii) Pattern-recognition: Giant T-U waves (especially post-pause) +/- "bizarre" bigeminy
(iii) Once you see this, determine the QT/U. If prolonged start treatment! (View Tweet)
- 13/ Treatment of Torsades deserves a separate discussion but some key points can be found here -
https://t.co/NSyn3JfMBK
https://t.co/ZSR6RsM8rI
Feel free to spread the word! (View Tweet)